






Description
Clinical History
A 74-year old male presented with a 2-month history of dysphagia, dysphonia, and weight loss. He had a history of heavy alcohol consumption and smoked 40 cigarettes per day for 40 years. Investigation discovered a laryngeal tumour. He received radiotherapy but his tumour recurred. He died 9 months after his initial presentation.
Pathology
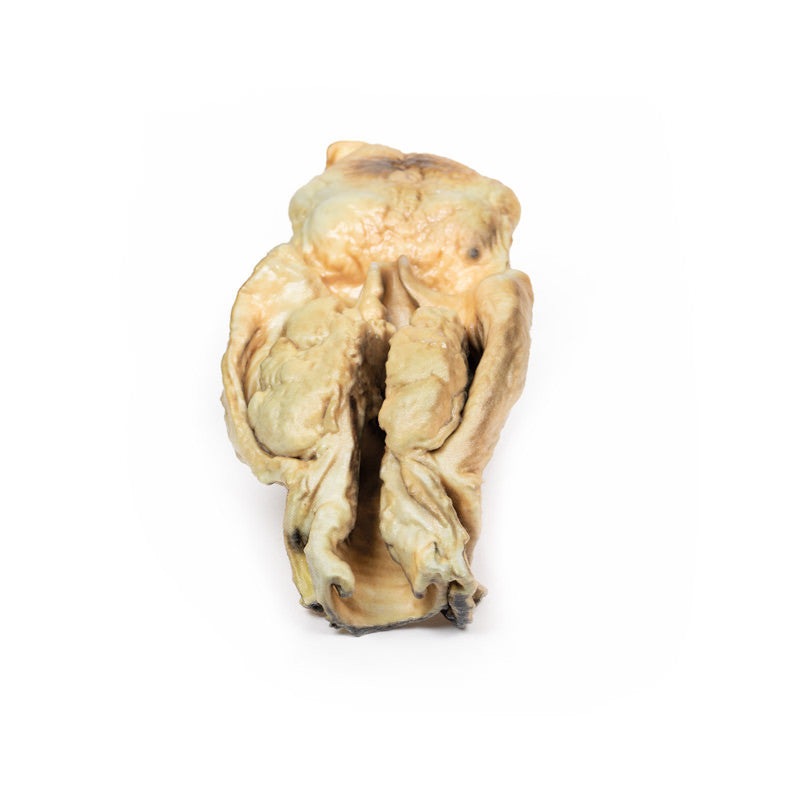
The specimen consists of tongue, pharynx, larynx, oesophagus, and trachea and has been mounted in the coronal plane. The oesophagus and trachea have been opened from the posterior aspect. There is a 5 x 4 x 2 cm fungating carcinoma evident extending into both pyriform fossae. The surface of the tumour is irregular with shaggy areas of necrosis. The tumour has arisen from the larynx and involves both vocal cords, the left aryepiglottic fold, and both pyriform fossae.
Further Information
Over 95% of laryngeal cancers are squamous cell carcinomas. The tumour usually develops on the vocal cords but may occur above or below the cords, on the epiglottis, aryepiglottic folds, or in the pyriform fossae. The cancer usually begins as squamous cell carcinoma in situ, progressing to ulcerated and fungating invasive carcinoma with continued exposure to carcinogens.
The greatest risk factors for developing cancer of the larynx are tobacco smoke and alcohol consumption. Human Papilloma Virus (HPV) infection, asbestos exposure, and irradiation have also been shown to be associated with increased incidence of head-and-neck squamous cell carcinoma (HNSCC). Males are affected more than females. It most frequently presents in the 6th decade of life.
Laryngeal cancer may spread by invading surrounding structures, via lymphatics usually to local cervical nodes, or haematogenous metastasis most commonly to the lungs. Common symptoms include dysphonia, dysphagia, odynophagia, globus sensation, and cough. Less commonly, haemoptysis, stridor, dyspnoea, and halitosis may be described.
Treatment varies depending on the stage of the disease. Smoking and alcohol cessation are important for all stages. Early disease laryngeal preservation treatments may include laser therapy, microsurgery, and radiotherapy. Later stage disease treatments may involve a combination of laryngectomy, radiotherapy, and chemotherapy.
HPV-related HNSCC have better outcomes than non-HPV positive tumours. HPV vaccination programs have been introduced in several countries, including Australia and the UK, for both boys and girls, to reduce their risk for HNSCC.
