








Description
Clinical History
In the 1970s, a 31-year-old woman presented with severe headache and diplopia on a background of having a pigmented skin lesion (diagnosed as an invasive skin melanoma) removed from her neck 8 months earlier. Clinical examination revealed no abnormality, and following discharge the patient was later re-admitted with persistent vomiting. Her condition deteriorated and she died.
Pathology
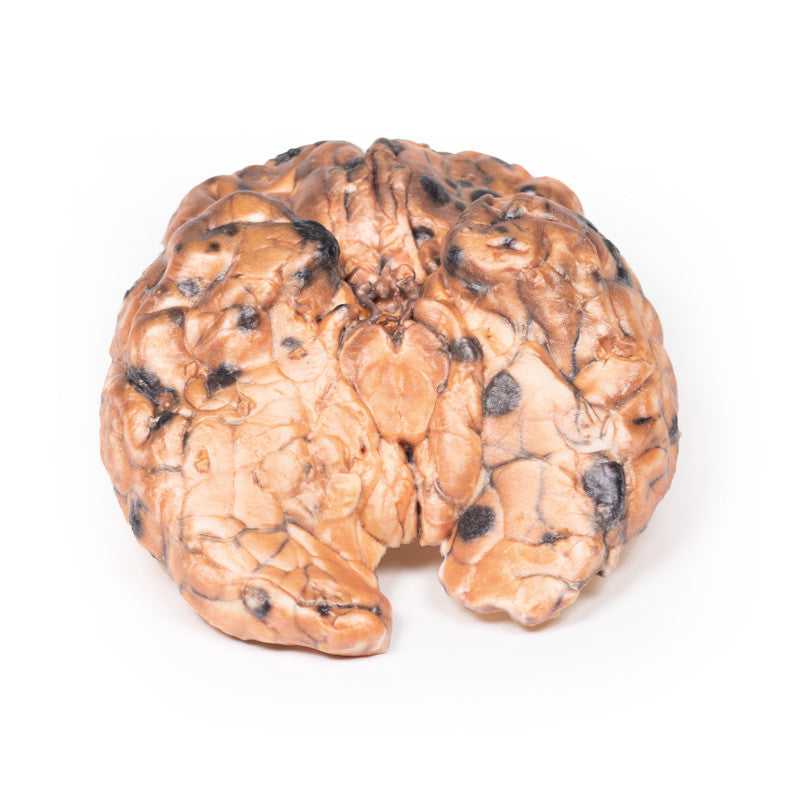
This specimen demonstrates widespread intracerebral melanoma metastases. The inferior surface is characterised by many elevated dark nodules up to 1.5 cm in diameter. Similar lesions are present on the cut superior surface where it is seen that these secondary melanotic deposits are confined exclusively to the grey matter. The tumour deposits are not encapsulated and are invading the cortex. Some necrosis and haemorrhage is present.
Further information
Of all patients who have metastatic disease to the brain, 10% are from skin melanoma. Risk increases with age over 60 years, male gender, disease duration and more advanced tumour/metastatic stage. BRAF and NRAS mutations, expression of CCR4 receptors on tumour cells, and activation of the PI3K pathway are all risk factors for the development of cerebral metastasis. 80% of melanoma brain metastases are supratentorial. Presentation is often with headache, neurologic deficits and/or seizures. Furthermore, these lesions are at risk of spontaneous haemorrhage. Modern diagnosis is based on neuroimaging and often histology of a stereotactic brain biopsy, if no previous diagnosis has been made. Treatment includes stereotactic radiosurgery (SRS), radiotherapy and/or systemic therapy with "checkpoint inhibitor immunotherapy" or targeted treatments. This has improved median survival up to 11 months in recent years.
