






Description
Clinical History
(pre access to CT and MRI imaging) This 51-year old woman had surgery for breast carcinoma 2 years before presentation. Her main complaint was left-sided ataxia for the 2 weeks prior, and this had been preceded by a fainting attack followed by left-sided weakness. Examination revealed a left spastic paresis. There was doubt as to the diagnosis because the rapidity of onset suggested a vascular lesion. She was discharged from hospital but six weeks after her initial presentation she was re-admitted with left-sided fitting. Lumber puncture and re-examination were not informative. EEG showed a right anterior temporal abnormality. Angiography confirmed the presence of a large space-occupying lesion in the right cerebrum. On the ward, there was a steady deterioration of the patient's condition, and ultimately death.
Pathology
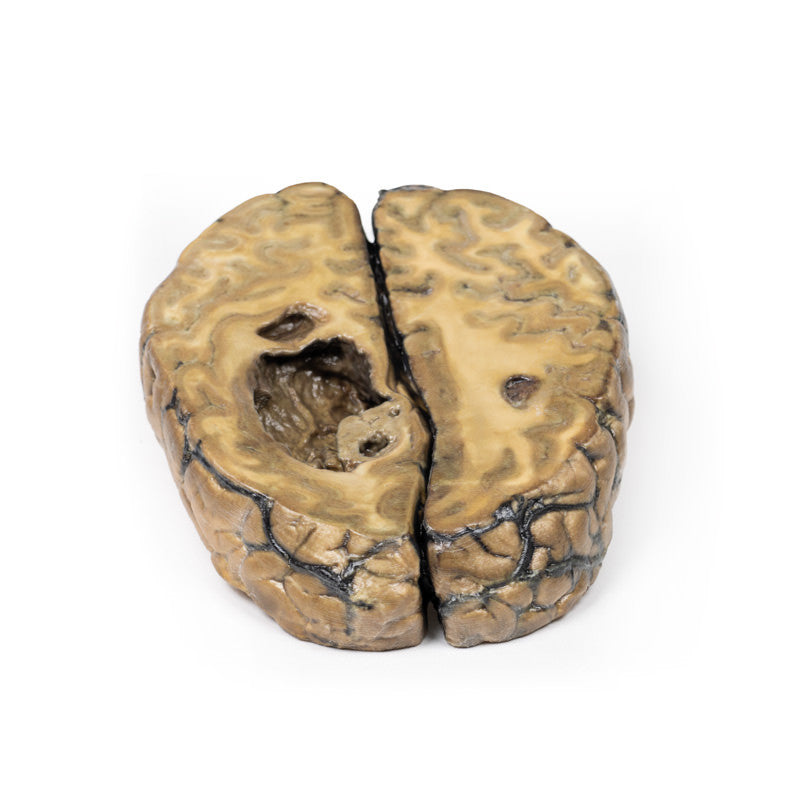
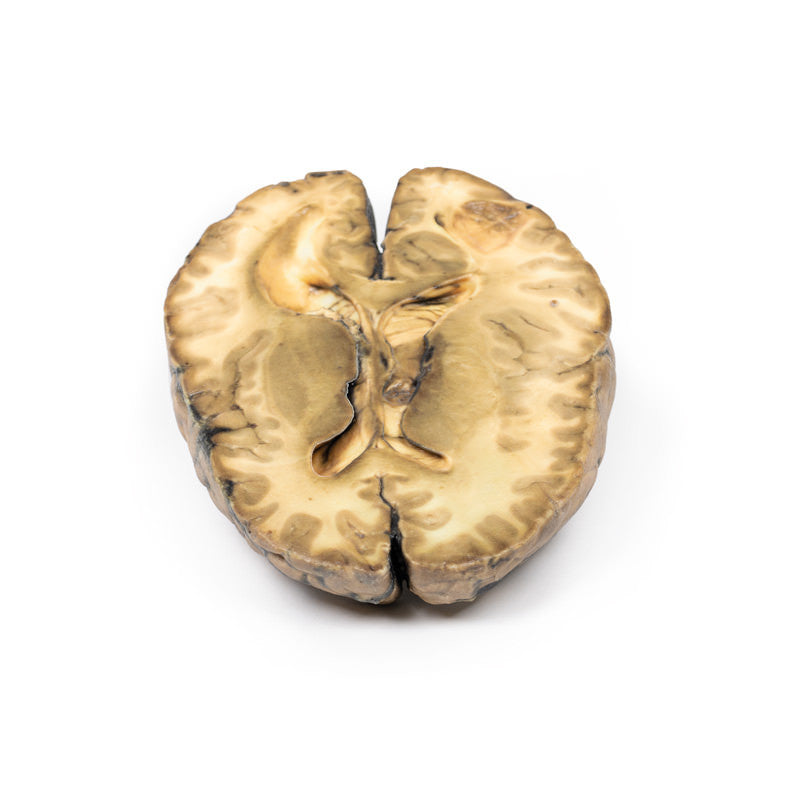
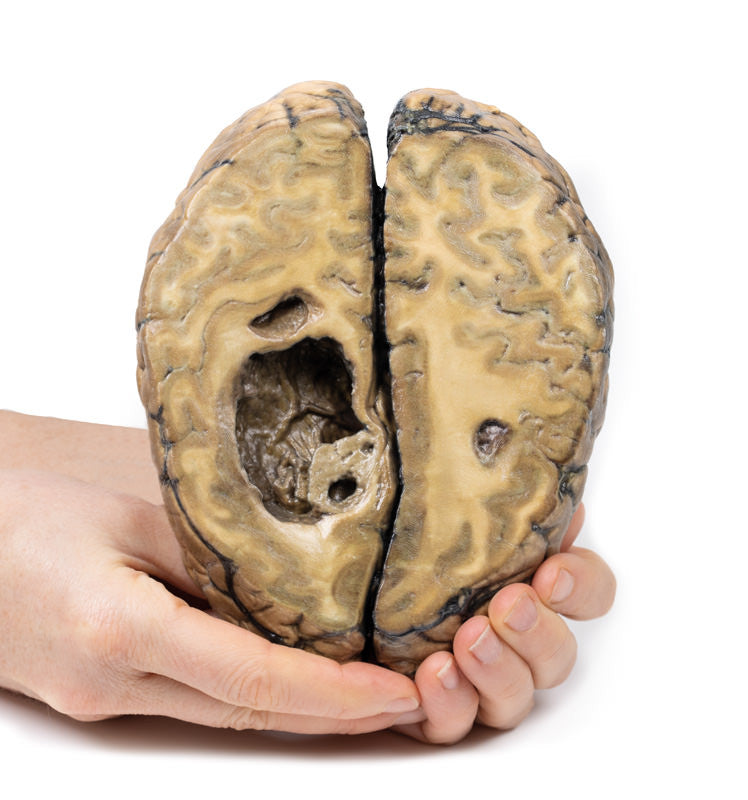
The specimen is the cerebrum sliced horizontally. On the superior view, the right hemisphere is clearly enlarged, particularly in the parietal region where the gyrae are widened and 3 cystic tumours are evident. The largest, 5 cm in diameter, is in the right parietal region. A smaller tumour, 2 x 1.5 cm in diameter, is seen close to the posterior margin of the largest tumour. A third one, 1.5 cm in diameter, is present in the left parietal region. The tumours have mainly involved white matter. The wall of each lesion is composed of shaggy friable greyish tissue. At necropsy, there was ulceration of the largest tumour into the right lateral ventricle (seen more clearly when the inferior surface is examined). Sub-falcine herniation was also seen, as is displacement of the basal ganglia and internal capsule. Histological examination revealed metastatic carcinoma in the viable areas. Other metastases were found in the liver and bone. Histology of a liver metastasis was consistent with origin from a primary carcinoma of breast.
