




Description
Clinical History
A 15-year-old boy with cough and sputum developed a hectic (spiking) fever and chest pain a few days before being admitted in a comatosed condition. Examination revealed an early diastolic murmur at the aortic area, which radiated down the left sternal edge. He deteriorated very quickly and died, despite antibiotic chemotherapy. Blood cultures grew Staphylococcus aureus.
Pathology
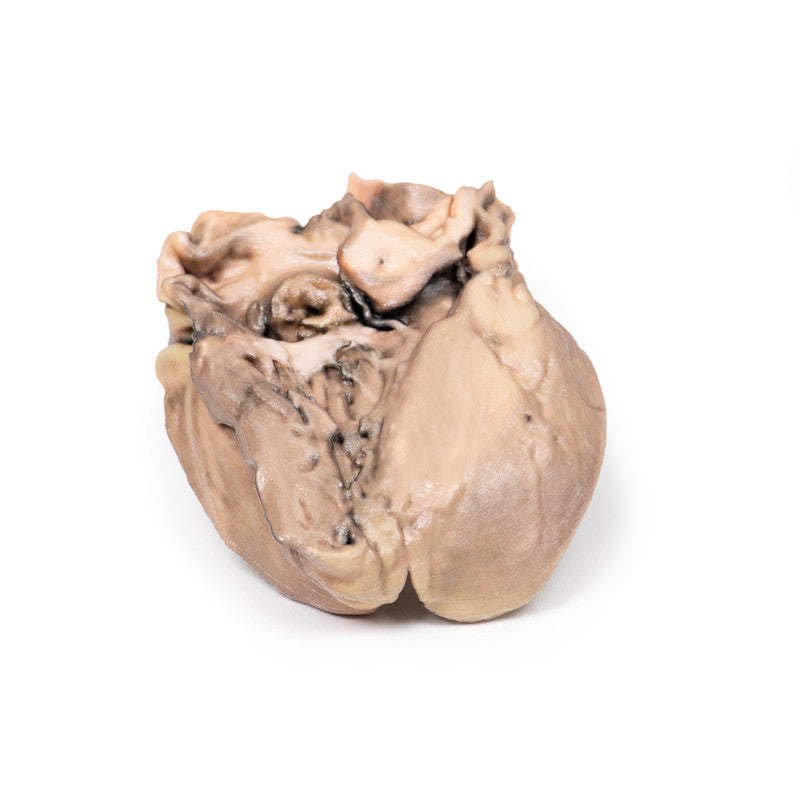
This small heart displays the left ventricle and associated valves. The non-coronary cusp of the aortic valve is ulcerated and perforated and has friable vegetations attached. Immediately below this cusp, a perforation extends into the right atrium just above the tricuspid valve (see back of specimen). The other aortic cusp is also thickened.
This is an acute bacterial endocarditis with aortic cusp and atrioventricular perforations.
Further Information
Acute bacterial endocarditis is a form of infective endocarditis. Endocarditis due to fungal infections can also occur, although they are rare.
In normal circumstances, the endothelial lining of the heart and valves is relatively resistant to infection by most bacteria or fungi. Therefore, in order for infective endocarditis to occur, there needs to be initial damage or injury to the endocardial tissue. This often results in aggregation of platelets and fibrin, which then become infected, resulting in vegetation formation (i.e. an infective nidus). Staphylococcus aureus, however, is highly virulent and can sometimes infect normal heart valves.
After the initial platelet-fibrin aggregation, there is further activation of the coagulating system via the extrinsic clotting pathway and initiation of the inflammatory response via monocytes, resulting in further growth of the vegetation/thrombus. The microbial growth tends to occur within the fibrin matrix, which makes it difficult for the immune responses to eradicate the infection. An additional problem is that these infected thrombi can also embolise, causing distant sites of infection in smaller capillaries (e.g. in the kidney).
Risk factors for developing an infective endocarditis include valvular heart disease, such as previous rheumatic heart disease, congenital heart disease (e.g. ventricular septal defect or bicuspid aortic valve), prosthetic heart valves, or any previous invasive cardiac procedures.
Anti-thrombotic medications – e.g. heparin or aspirin – may have to be administered in patients at risk. Diagnosis is initially made by clinical examination followed by pathology (blood cultures) and diagnostic imaging. Transthoracic echocardiogram is often first line, followed by transoesophageal echocardiogram.
Treatment includes antimicrobial therapy, anti-coagulants, and in some complicated cases, surgical intervention such as valve surgery.
